
Merkel cell carcinoma
This rare aggressive neuroendocrine skin cancer is associated with pathogenic factors
such as UV exposure, immunosuppression, and/or Merkel cell polyomavirus. It presents
as a rapidly growing bluish red or skin-coloured nodule, usually on a sun-exposed site,
and spreads quickly to the lymph nodes, lungs, liver, or bone.

Dermatofibrosarcoma protuberans
A slow-growing, locally recurrent cutaneous soft tissue sarcoma caused by a
chromosomal translocation t(17;22)(q22;q13) which results in a COL1A1–PDGFB fusion
gene. Presents as an asymptomatic ‘scar’ or a violaceous, reddish brown, or skin-
coloured nodule or plaque, which feels rubbery or firm. has an infiltrative pattern, often
with considerable subclinical and asymmetrical extension.
Treatment: surgical excision (1–3cm peripheral margins) or Mohs micrographic surgery.
Rarely metastasizes (<5%).

Paget disease
Paget disease is caused by direct extension of a mammary intraductal adenocarcinoma
into the skin of the nipple or areola.

Metastatic disease
Skin metastasis may be the first sign of an internal malignancy. The skin may be
infiltrated by direct invasion of tumour cells or by spread from lymphatics or blood
vessels. The tumour may also be implanted into surgical scars. Cancers most often
associated with cutaneous metastasis are:
• Breast: skin of the chest, scalp, (rarely eyelid).
• Stomach, colon: skin of the abdominal wall, especially periumbilical.
• Lung: skin of the chest, scalp.
•Genitourinary system (uterus, ovary, kidney, bladder): skin of the scalp, lower abdomen,
external genitalia.
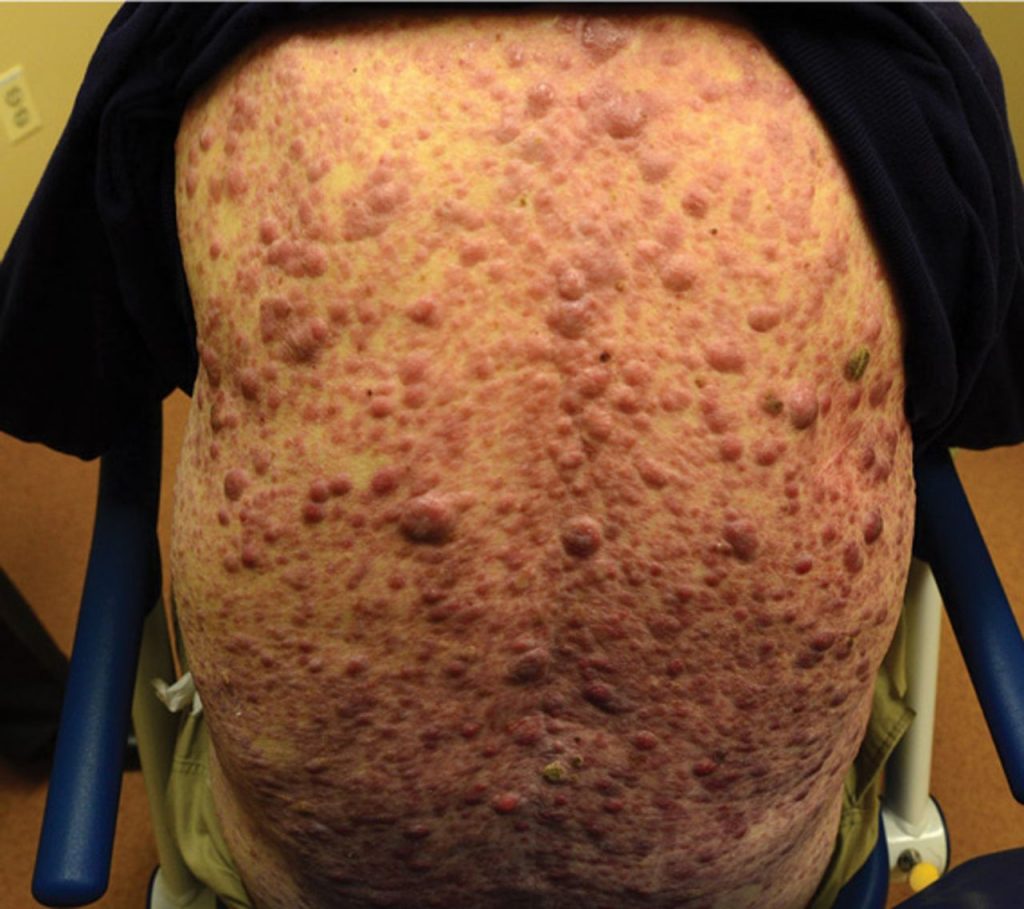
Leukaemia cutis
Leukaemia cutis is rare but is seen most often with myeloid leukaemias, e.g. acute
monocytic or myelomonocytic leukaemias. Cutaneous deposits may precede the
transformation of myelodysplastic syndrome to leukaemia. It usually indicates a poor
prognosis.
Primary cutaneous B-cell lymphomas
Most B-cell lymphomas affecting the skin are systemic.
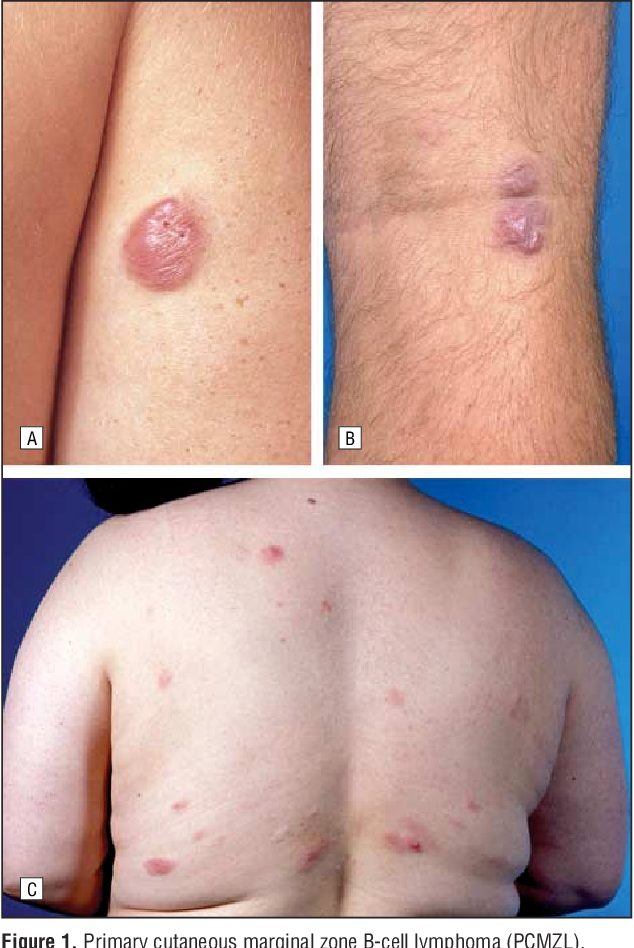
* Marginal zone lymphoma (mucosa-associated lymphoid tissue, MALT).
• Dermal tumours in male affecting the trunk and upper limbs.
• Indolent and prone to recur.
• Test for Borrelia burgdorferi.
• Radiotherapy is the treatment of choice.
* Follicular lymphomas:
• Multiple primaries, prominent plaques affect scalp and upper trunk.
• Treat with radiotherapy or rituximab.
• 95–100% 5-year survival.
* Diffuse large B-cell lymphoma:
• Leg-type seen in older female.
• Large, rapidly growing, bluish red tumours.
• 50% 5-year survival.
• Treatment is with radiotherapy/CHOP–rituximab.