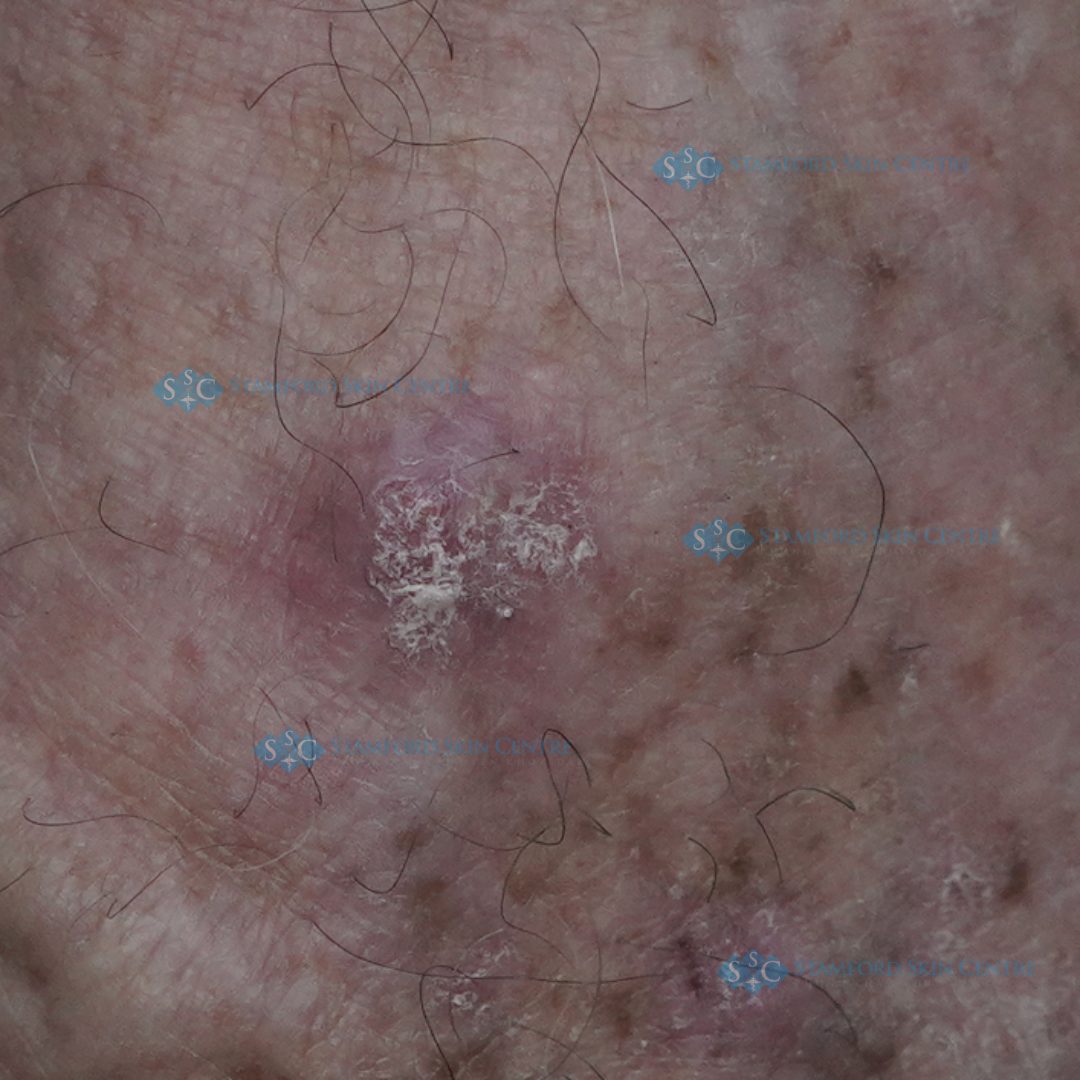
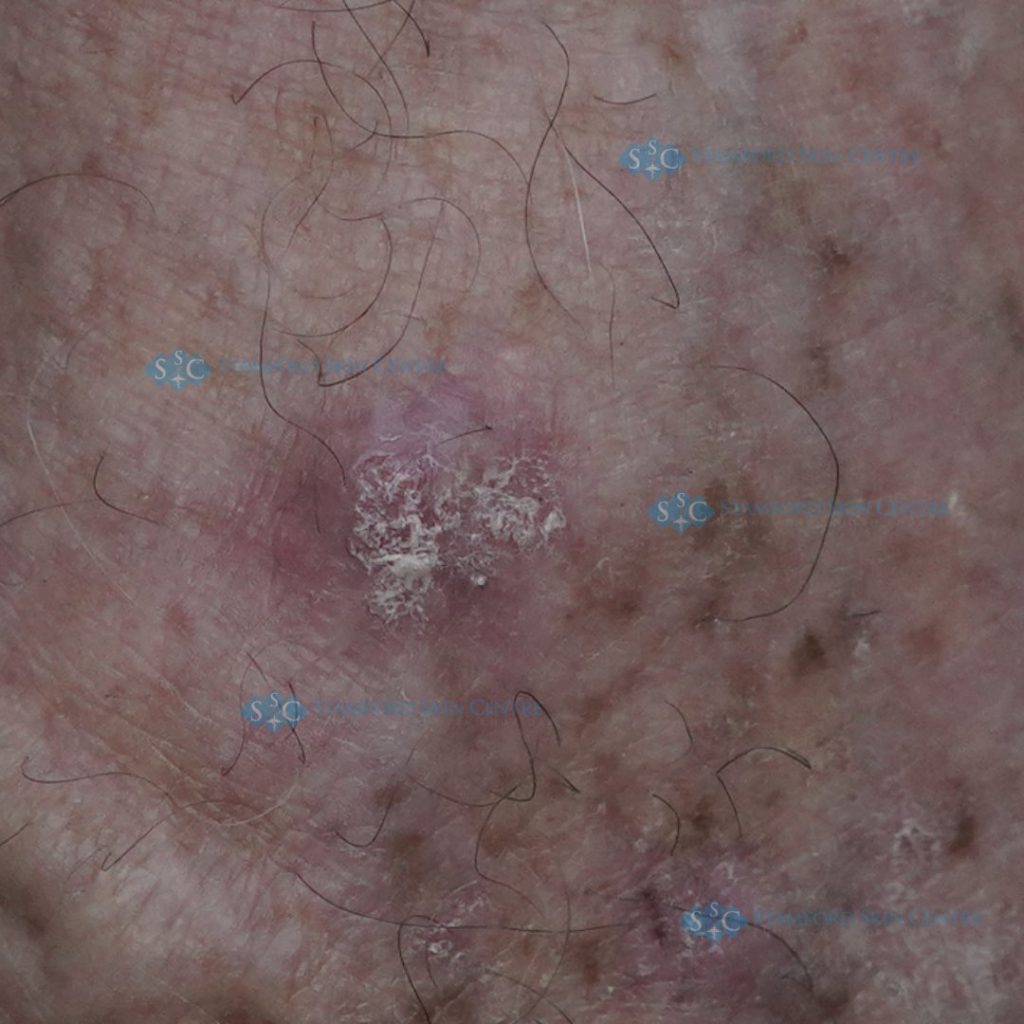
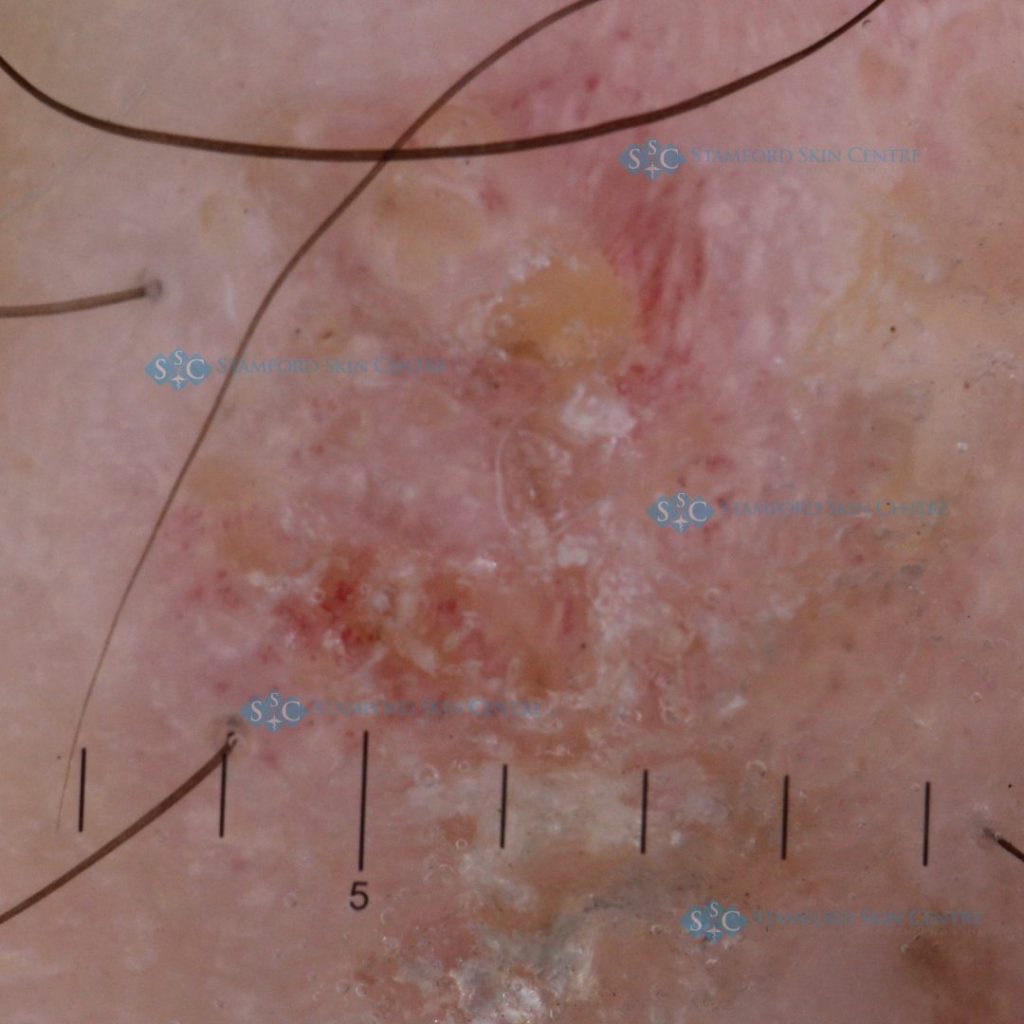
Male patient, 67 years old, with a history of many previous excisions of skin cancer
lesions. One year recently, a new skin lesion has developed on the dorsal of foot, clinical
diagnosis was Actinic keratosis. The lesion is excised according to the patient's wishes,
resulting in Invasive Moderately Differentiated Squamous cell carcinoma.
The differential diagnosis of squamous cell carcinoma includes actinic keratosis,
amelanotic melanoma, basal cell carcinoma, benign tumors, keratoacanthoma, healing
traumatic wounds, spindle cell tumor and warts.
Squamous cell carcinoma is the second most common skin cancer, comprising 20 percent
of all cases of nonmelanoma skin cancer. This is the most common tumor in elderly
patients, and it is usually the result of a high lifetime cumulative dose of solar radiation.
However, other irritants and exposures may lead to squamous cell carcinoma. Up to 60
percent of squamous cell carcinomas occur at the site of a previous actinic keratosis.
Changes in an actinic keratosis that suggest evolution to squamous cell carcinoma include
pain, erythema, ulceration, induration, hyperkeratosis and increasing size.
Squamous cell carcinomas may grow aggressively and are associated with a 2 to 6
percent risk of metastasis. Risk factors for metastasis include poor cell differentiation,
increasing lesion depth and location on the lip or ear. The most common locations for
metastatic spread are the regional lymph nodes, lungs and liver. Once metastasis occurs,
the five-year cure rate for squamous cell carcinoma is 34 percent. Recurrence and
metastasis typically occur within three years of initial treatment.
For more information, please visit : https://stamfordskin.com/en/dermatology/squamous-
cell-carcinoma/