Vascular damage may occur in infective endocarditis, meningococcaemia, chronic
gonococcaemia, Gram-negative septicaemia, and rickettsial infections. Septic vasculitis
can also follow any intravascular procedure.
The vasculitis tends to involve both small and medium-sized vessels. organisms damage
blood vessels by direct invasion, release of endotoxins that provoke thrombosis (DIC),
and immune complex-mediated vasculitis.

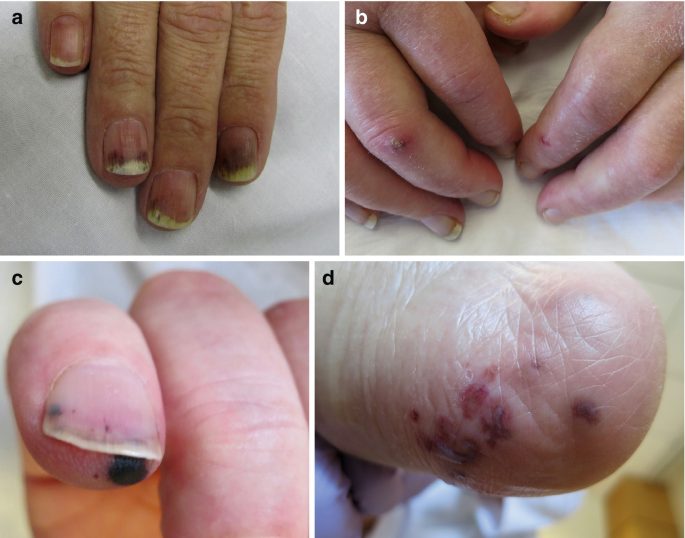
1. Infective endocarditis
Signs include splinter haemorrhages in nails, mucosal petechiae, osler nodes (tender,
erythematous spots on the pulps of fingertips and toes), and Janeway lesions (non-tender
red or haemorrhagic macules or nodules on the palms and soles). Skin manifestations are
associated with a high risk of complications, e.g. cerebral emboli.
2. Acute meningococcaemia
A life-threatening illness that must be treated immediately with IV antibiotics, e.g.
cefotaxime 2g. Purpuric lesions develop on the limbs or trunk within 12–36h of the onset
of infection. These may be small and few in number. Purpura fulminans with DIC is a
devastating complication.
Fibrin thrombi occlude capillaries, venules, and vessels in the deeper dermis and
subcutis, leading to ischaemia and infarction. Persistent cyanosis of the extremities is an
early warning sign. Large, irregular, indurated ecchymoses become necrotic, blister, and
may progress to extensive gangrene.
3. Gram-negative septicaemia (Escherichia coli, Pseudomonas, or Klebsiella)
Septic emboli produce erythematous wheals and papules that become irregularly purpuric
and necrotic.
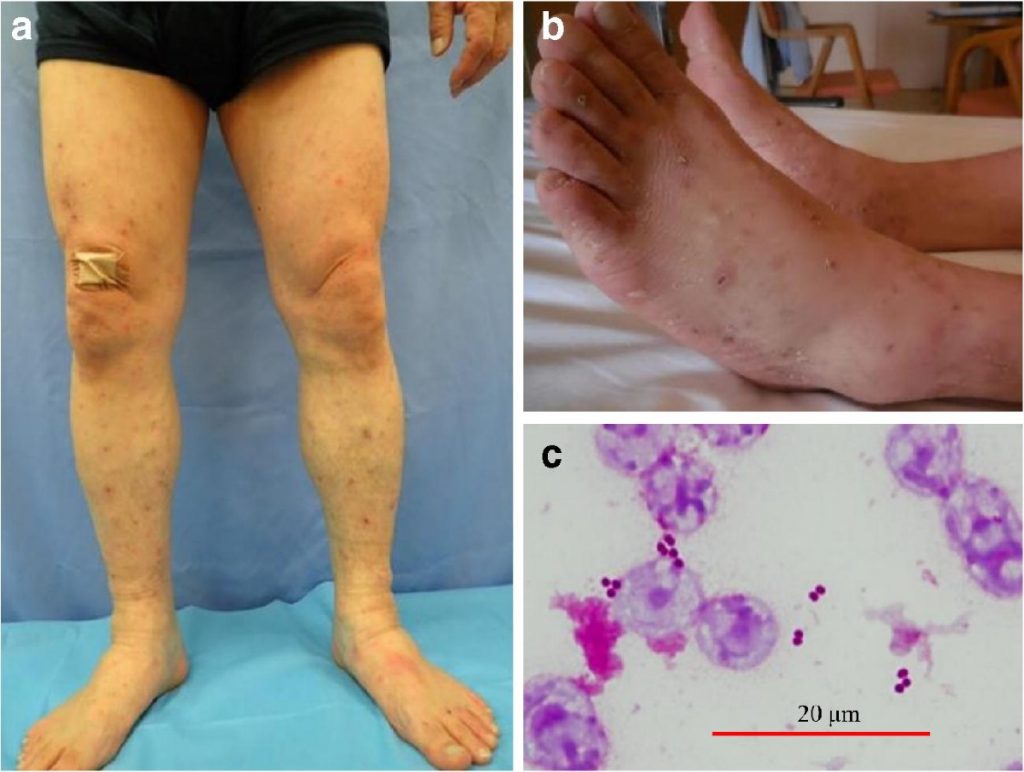
4. Chronic meningococcaemia and chronic disseminated gonococcaemia
Rare immune complex-mediated illnesses associated with fever, arthralgia, arthritis, and
a cutaneous vasculitis. Look for scattered purpuric papules and vesicopustules on the
trunk and extremities (meningococcaemia) or the palms, fingers, and toes
(gonococcaemia). These may be few in number.
5. Rocky Mountain spotted fever
Rickettsia rickettsii invades the walls of small cutaneous vessels, inducing a focal
lymphocytic vasculitis. Look for an erythematous maculopapular rash that becomes
petechial and purpuric within 24–48h.

6. Septic vasculitis after percutaneous arterial puncture
Signs suggest unilateral cutaneous emboli: local infarction, livedo, and/ or retiform purpura.