
Skin cancer, lymphoma/lymphoproliferative malignancies, and solid organ tumours are
common in renal transplant recipients (RTRs) and are a leading cause of death. By 5
years after transplantation, the risk of developing an SCC is 7100 times greater than in an
immunocompetent patient. Most patients have multiple cancers. Pathogenesis of skin
cancer is multifactorial. Risk relates to the level, as well as chronicity, of
immunosuppression, e.g. patients who receive cyclosporin, prednisolone, and
azathioprine have a three times higher risk of SCC than those taking prednisolone and
azathioprine alone. Switch of immunosuppressant drugs to mycophenolate mofetil and
sirolimus may reduce the risk of future cancers but risk compromising graft function.
T-regulatory (Treg) cells (a subset of T-lymphocytes) suppress immune responses
(facilitating cancer development) and inhibit graft rejection. There is now strong evidence
for a potentially causal relation- ship between Treg cell numbers and cancer incidence in
RTRs.

What should I look for?
• Photodamage: telangiectasia, solar elastosis, erythema, pigmentation. Common in fair-
skinned individuals who are at greatest risk of skin cancer.
• Persistent HPV-induced warts and pre-cancers, e.g. Bowen disease, solar keratoses on
sun-exposed skin. Large numbers of seborrhoeic warts are linked to an increased risk of
skin cancer.
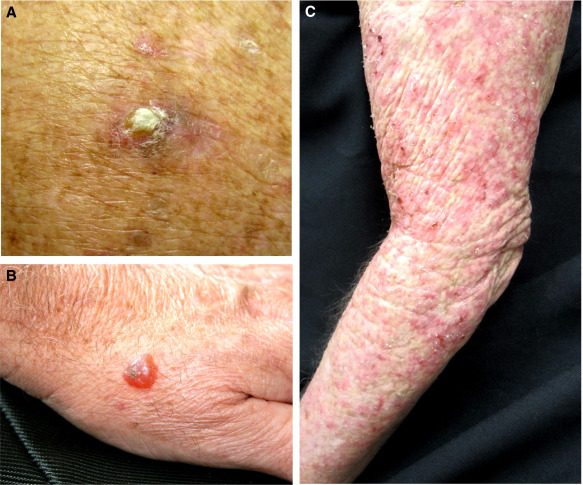
• New warty papules or tender keratotic nodules on sun-exposed skin: SCCs are the
commonest skin cancer (65- to 250-fold increase in risk) and may resemble viral warts.
SCCs are significantly commoner in immunosuppressed patients than BCCs, a reversal of
the usual ratio of three BCCs to one SCC. RTRs with SCC are at increased risk of
developing internal malignancies.
• Other skin cancers include BCC (10- to 16-fold increase), malignant melanoma (3- to 8-
fold increase), KS (84-fold increase, hhV-8- related), and Merkel cell cancer
(polyomavirus-related).
• Non-melanoma skin cancers are commoner in fair-skinned individuals living in tropical
or subtropical countries.
• Post-transplant lymphoproliferative disorders (mostly B-cell/EBV- related) rarely
present in skin with erythematous patches or nodules.
Symptoms :
• Clinical accuracy of diagnosis is poor: cancers may appear banal, but conversely warts
or hypertrophic solar keratoses may simulate SCC. Have a high index of suspicion, and
biopsy or excise changing lesions for histological examination, particularly new tender
nodules on sun- exposed skin. Cancer on the lip and ear may be subtle.
• Ensure the patient understands the importance of rigorous sun protection, and reinforce
the message regularly.
• Ensure that patients with chronic kidney disease, who may eventually need a transplant,
are educated about the importance of sun protection and regular self-examination.
• Examine all the skin of transplant recipients regularly; patients are best managed in
dedicated transplant/immunosuppressed skin clinics.
• Oral acitretin 10–25mg/day may reduce the incidence of skin cancers.
• High-risk primary skin cancers/locally invasive disease should be managed by reducing
immunosuppression which must be undertaken with guidance from renal transplant
physicians.