
Clinical features, in combination with histological, immunophenotypic, and molecular
studies, have helped to delineate subtypes and provide prognostic criteria in this
heterogeneous group that includes:
• MF and Sézary syndrome.
• CD30-positive CTCLs, e.g. lymphomatoid papulosis—good prognosis. Anti-CD30
monoclonal antibodies (brentuximab) now available as a treatment option.
• CD30-negative CTCLs: poor prognosis.
• Adult T-cell leukaemia/lymphoma (ATLL).
Mycosis fungoides
MF, the commonest CTCL, is a malignancy of effector memory T-cells that responds
well to skin-directed therapies. The aetiology is uncertain but may involve chronic
antigenic stimulation (possibly viral) and mutations in oncogenes or DNA repair genes.

Disease is indolent, and the diagnosis often delayed (median age 55–60 years).
Prognosis is worse in patients aged >60 years and in late-stage disease.
MF progresses through three stages: patches, plaques, and tumours— which may overlap.
MF variants include folliculotrophic, pagetoid reticulosis, and granulomatous slack skin.
early-stage disease (excellent prognosis) is managed conservatively. Options include
emollients, potent topical corticosteroids, UVB, PUVA, topical nitrogen mustard, and
bexarotene (retinoid that activates retinoid X receptors, causing T-cell apoptosis).
radiotherapy is effective for localized thick plaques or tumours. MF is relatively
chemoresistant, and treatment of advanced dis- ease is unsatisfactory. Sepsis is a common
cause of death.
Sézary syndrome
This form of CTCL accounts for about 5% of new cases. It is caused by malignant
proliferation of central memory T-cells. Disease is characterized by erythroderma,
lymphadenopathy, and malignant circulating CD4+ T-cells (Sézary cells) forming >5%
of the total lymphocyte count. The CD4:CD8 ratio is high (≥10). As disease progresses,
the malignant clone of cells expands, and the normal CD4 (T-helper) and CD8 (T-
suppressor) populations decrease.

Prognosis is poor (median survival 32 months from diagnosis), and patients often die
from infection as a result of a failing immune system. Treatment is unsatisfactory; PUVA
is poorly tolerated. Options include extracorporeal photophoresis, multi-agent
chemotherapy, immunotherapy, and oral bexarotene, but prospective clinical trials are
needed.
Adult T-cell leukaemia/lymphoma
This CD4+ lymphoproliferative disorder, associated with infection with HTLV-1, is
commonest in Japan and the Caribbean. Prognosis is poor, and opportunistic infection
common.
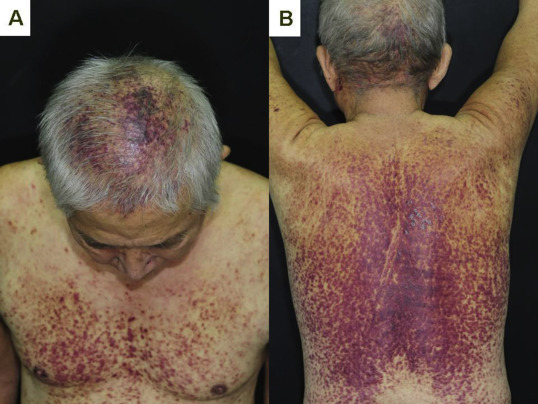
What should I look for?
• Skin infiltration by ATLL cells leads to patches, plaques, papules, or tumours. Rarely
erythroderma or purpuric rashes.
• Non-specific cutaneous inflammation (dermatitis) and infections, e.g. dermatophyte
(tinea), Candida.
• Lymphadenopathy, hepatosplenomegaly.
• Raised LDH and hypercalcaemia.