What is erythema nodosum?
• EN is the commonest type of panniculitis. It is a septal panniculitis. Vasculitis is not a
feature of typical EN.
• EN may be a delayed hypersensitivity response to infection or to an underlying
inflammatory disease, but no cause is identified in about 1/3 of cases. Cases usually occur
in the first half of the year, possibly because of an increase in streptococcal infections.
• Most cases appear between the second and fourth decades, with a peak incidence
between the ages of 20 and 30. EN is commoner in women.
• Prognosis depends on the underlying disease. Idiopathic EN is self- limiting with an
excellent prognosis. Relapses are uncommon.

What should I look for?
• Underlying triggers.
• A prodrome with fever, malaise, arthralgia, and headache.
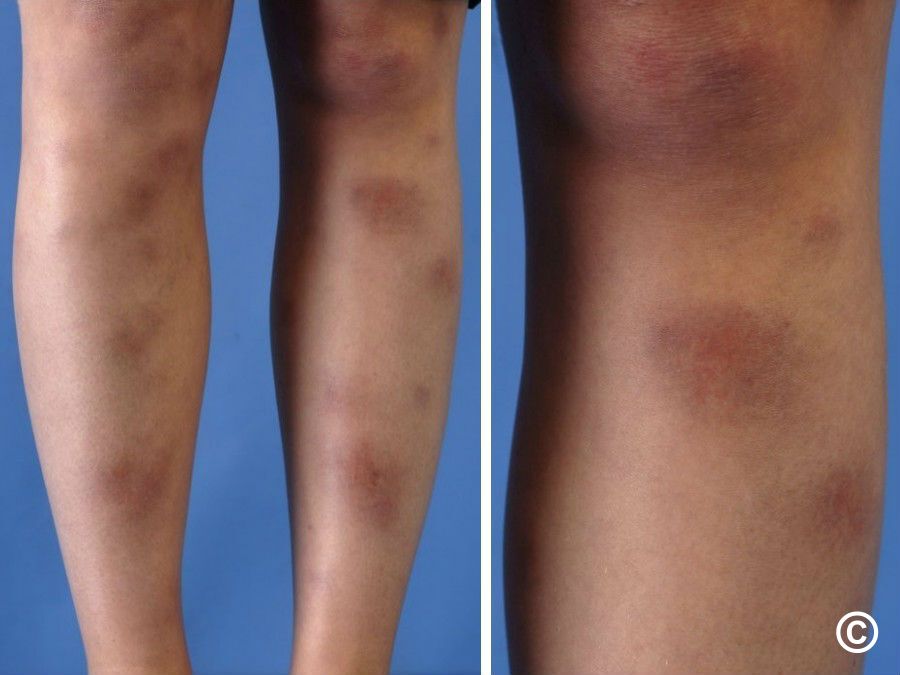
• Tender, erythematous (no purpura), warm nodules, measuring 1–5cm or more in
diameter.
• A symmetrical distribution on the shins, ankles, and knees.
• Less often, nodules appear on the arms or trunk.
• EN does not ulcerate.
• Sometimes GI problems such as abdominal pain, vomiting, or diarrhoea.
• Nodules fade over 2–6 weeks (more quickly in children), leaving a purplish, bruise-like
appearance that slowly resolves.
• Absence of scarring (nodules do not leave a depression—contour goes back to normal).
• A chronic migratory variant (subacute nodular migratory panniculitis, erythema
nodosum migrans) is much less common and usually presents as a single tender,
indurated, erythematous plaque that slowly enlarges peripherally, while clearing
centrally.
What should I do?
• Check FBC, ESR, urinalysis, and chest radiography.
• Further investigations should be guided by the history, examination, and local
prevalence of aetiological factors such as bacterial, viral, fungal, or protozoal infections.
• If required, take a deep elliptical biopsy that includes fat (a biopsy is usually
unnecessary).
• Manage any underlying problem such as infection.
• Provide pain relief with NSAIDs.
• Elevation may relieve pain in acute disease.
• Support stockings control swelling and may speed resolution.
• Potassium iodide 300–900mg/day has been recommended in persistent disease.
• Rarely, oral corticosteroids are required, but exclude an infection before prescribing.