
Behçet disease is rare, chronic, multisystem, and relapsing. the pathogenesis is not
understood but involves immune complex-mediated vasculitis. Most commonly affects
populations along the ‘silk route’ in turkey, Iran, and Japan but is seen worldwide.
Associated with HLA-B51. Diagnosis based on clinical criteria.
What should I look for?
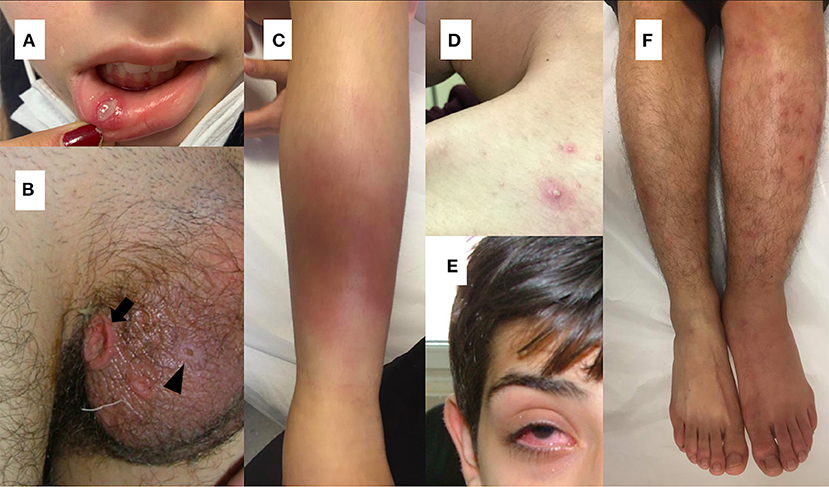
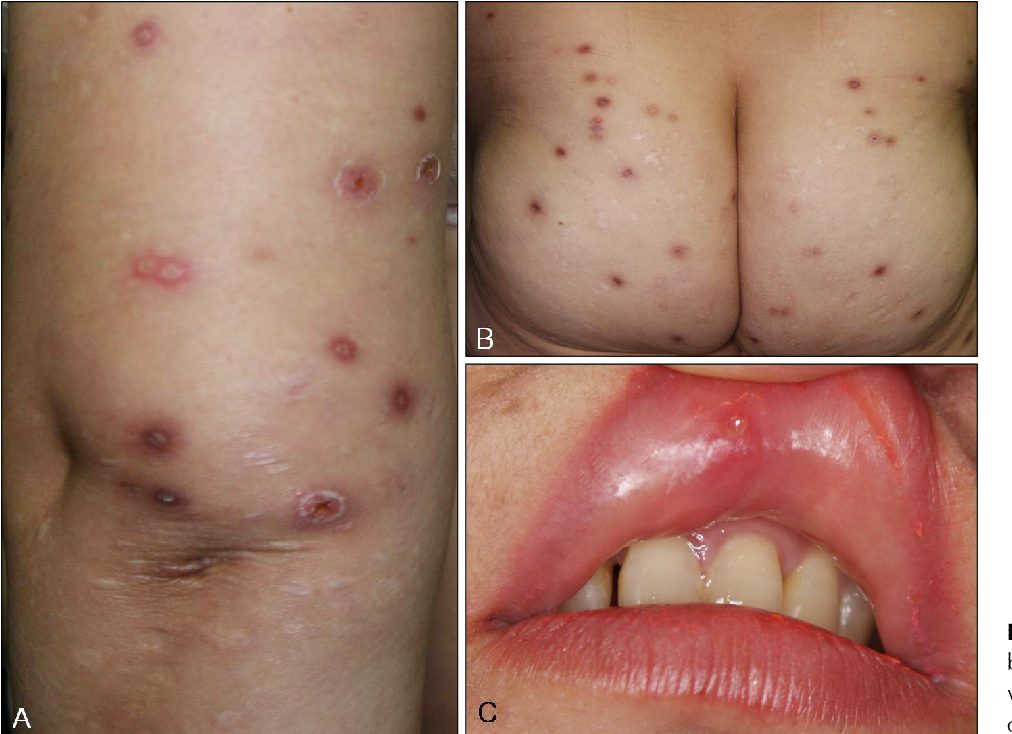
Mucocutaneous lesions
• Oral ulceration (all patients): recurrent and painful; small ulcers heal without scarring,
but larger ulcers may scar.
• Genital ulceration (85% of patients): usually scrotal or labial, may affect the vagina and
cervix, usually leaves scars.
• Papulopustular lesions (85% of patients): resembling acne or folliculitis, appear as
papules on an erythematous base, and develop into a pustule over 24–48h. Commonest
on the trunk.
• EN-like lesions (50% of patients) on legs. resolve, leaving pigmentation.
• Superficial thrombophlebitis (25% of patients): erythematous, tender, subcutaneous
nodules in a line. May be confused with EN.
• Extragenital ulceration: uncommon but may occur at any site.
• History of pustules developing at sites of needle-prick (pathergy), e.g. 24–48h after
venepuncture.
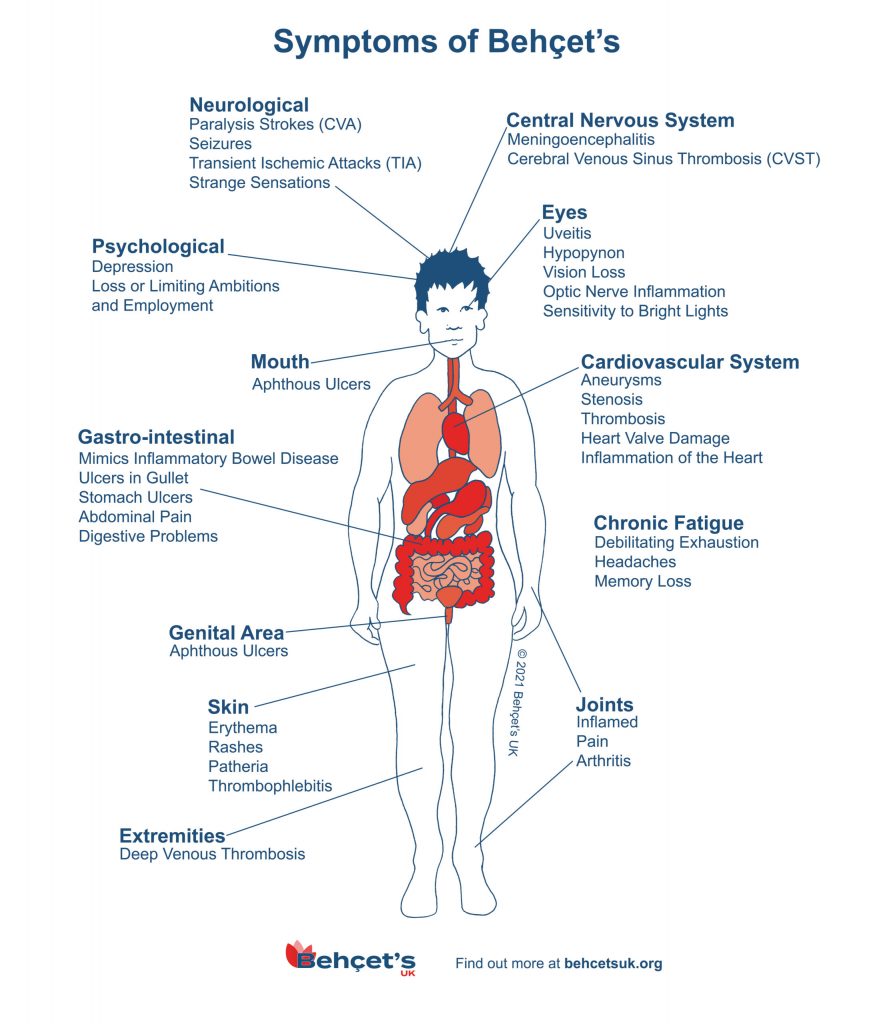
Eye disease (50% of patients)
• Chronic, relapsing anterior and posterior uveitis. Major cause of morbidity. May result
in retinal haemorrhage, papilloedema, and macular disease, with loss of visual acuity and
threat of blindness.
Musculoskeletal disease (50% of patients)
• Most often a non-deforming, non-erosive peripheral oligoarthritis, lasting a few weeks.
• Some patients have chronic arthritis, osteonecrosis, and myositis.
Neurological disease (5% of patients)
• Pyramidal, cerebellar, and sensory signs, sphincter disturbance, behavioural changes,
and dural sinus thrombosis.
• Peripheral nerve lesions are unusual.
Vascular disease (5% of patients)
• Large-vessel vasculitis can result in thrombosis and occlusion.
Other systems (rare)
• GI mucosal ulceration, splenomegaly, glomerulonephritis, and cardiac involvement
have been reported.
What should I do?
Investigations
• Pathergy test: hyper-reactivity of the skin to needle-prick (skin-prick of the forearm
results in a papule or pustule in 24–48h). Sensitivity varies (~60%) and is highest in
Japan and Mediterranean countries, but is highly specific for Behçet disease.
• Biopsy: papulopustular lesions or pathergy reactions.
• Genital ulcers: exclude infection, e.g. herpesvirus, EBV.
• FBC may show anaemia of chronic disease and leucocytosis.
• Inflammatory markers are not good indicators of disease activity.
• ANA, RF, and anti-neutrophil cytoplasmic antibody (ANCA) are negative.
Treatment
• A very potent topical corticosteroid ointment (clobetasol propionate) and topical 2%
lidocaine gel may relieve pain in oral and genital ulcers.
• Refer to ophthalmology for eye symptoms or signs.
• Colchicine may reduce arthralgia and mucocutaneous lesions.
• The use of systemic corticosteroids is controversial.
• Other immunosuppressives used include azathioprine, ciclosporin,
methotrexate, mycophenolate, and cyclophosphamide.
• Anti-TNF biologic agents infliximab, adalimumab, and etanercept may be effective in
severe disease.
• Thalidomide can be effective for aphthous ulcers but has been replaced by the use of
biologics.
• Interferon alfa may have a role in oral and genital ulcers.