LP is a chronic inflammatory condition of unknown cause that may affect mucosal
surfaces and/or the skin. A band-like ‘lichenoid’ infiltrate of lymphocytes hugs the basal
layer of the epidermis or epithelium.
LP can be drug-induced. Infrequently oral LP is caused by allergies to metals or
flavourings in foods.
What should I look for?
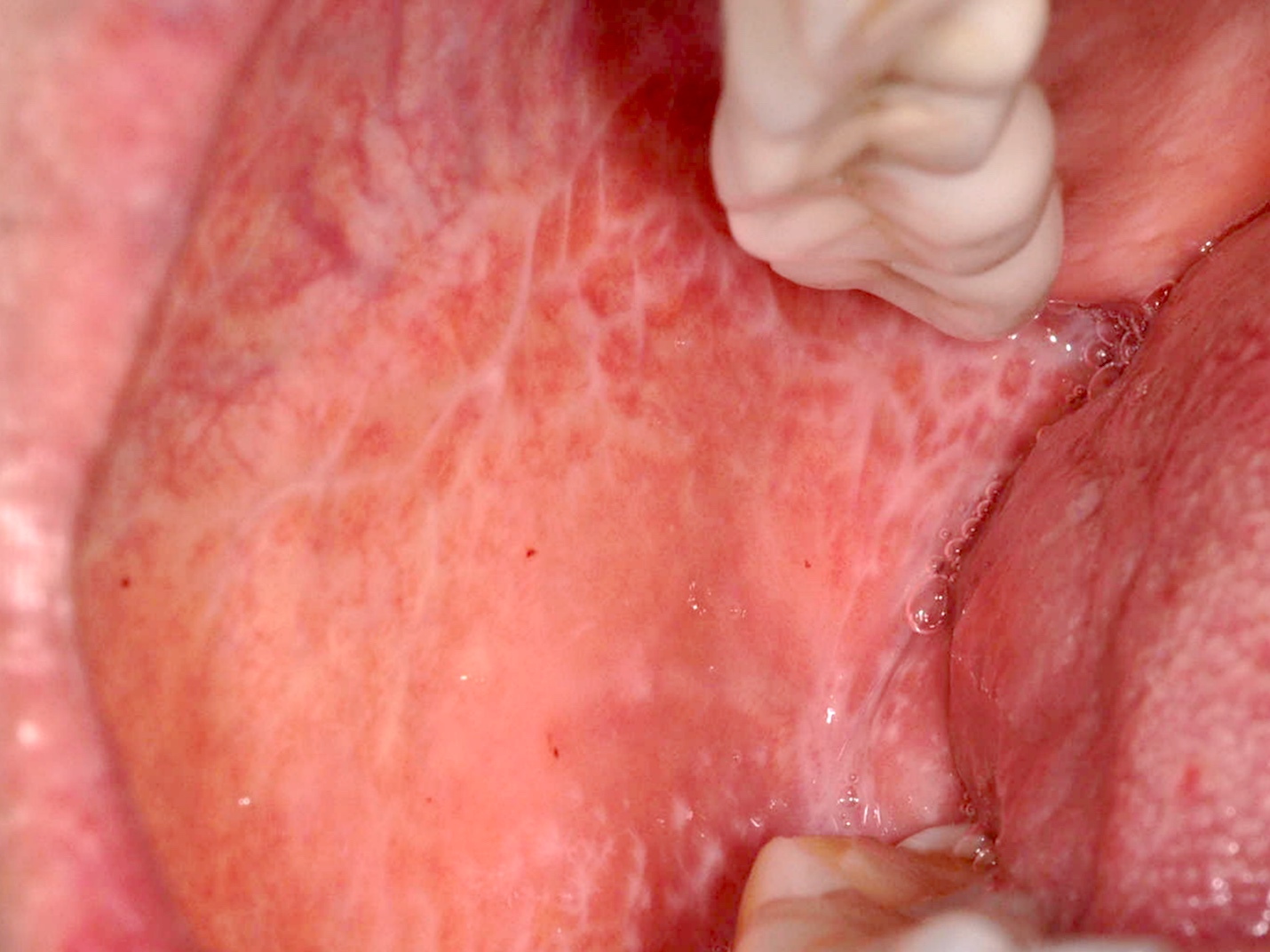
• Asymptomatic lacy white streaks (Wickham striae), and white papules and plaques on
the buccal mucosa, tongue, or genitalia (vulva, glans penis, shaft of the penis). these
cannot be scraped off, unlike mucosal candidiasis.
• Erosive mucosal disease: glazed erythema, erosions with white lacy border, painful oral
ulcers. May also have erosive genital disease— vulvovaginal–gingival syndrome, peno-
gingival syndrome.
• Gingivitis (erythematous erosions, patchy hypopigmentation).
• Genital lesions may become hypertrophic.
• Annular LP on the shaft of the penis may be associated with flexural annular LP, e.g. in
axillae.
• Erosive vulvovaginal LP (vulvar vestibule and vagina) with itch, dysuria, and/or
dyspareunia. Associated with oral disease, especially gingival LP.
• Scarring in chronic erosive vulvovaginal disease, with atrophy and fusion of the labia
and narrowing of the vaginal introitus.
• SCC is a rare complication in chronic erosive disease and may be asymptomatic—check
for mucosal thickening, a nodule, or a persistent ulcer.
• Cutaneous disease: flat-topped, shiny polygonal purplish papules. Seen more often in
oral and penile LP than vulval LP.
• Rarely, LP affects the oesophagus, larynx, bladder, and/or anus.
What should I do?
• A biopsy may be required to confirm the diagnosis.
• Consider taking swabs for viral culture from painful erosions.
• Withdraw any potentially causative systemic drugs.
• Oral LP: consider patch testing to exclude allergy to metals or oral flavourings (rarely
positive).
• Erosive mucosal disease may be chronic and persistent: patients should be counselled
about the risk of SCC and reviewed regularly.
Differential diagnosis
• Chronic cutaneous GVHD shares many clinical and histological features with LP.
• Oral DLE can look similar to oral LP.
• Vulval LP may simulate lichen sclerosus